
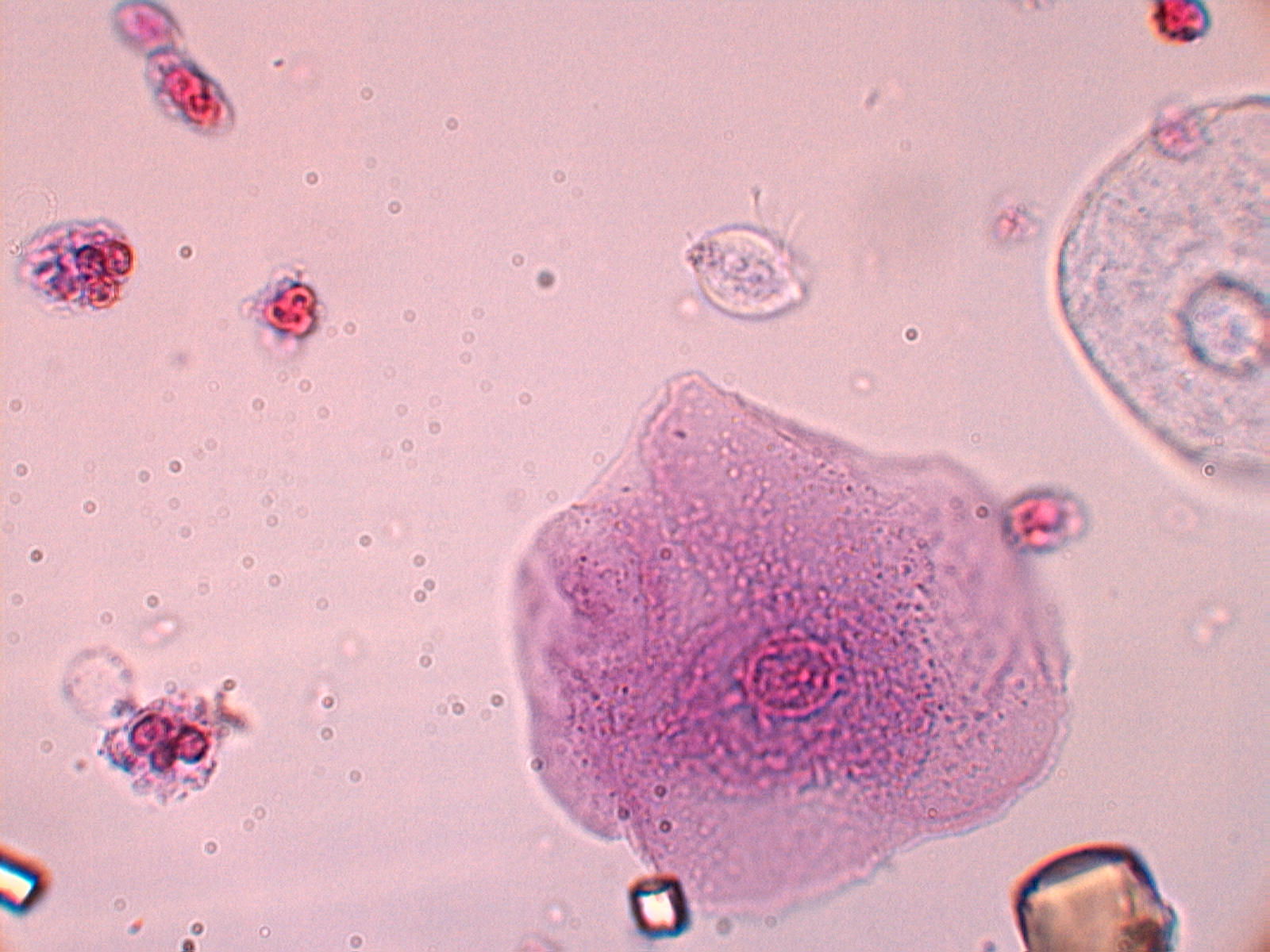
The organism in the photo was identified by a Medical Technologist as Trichomonas vaginalis.
IDENTIFICATION & DETECTION METHODS

photo by W. Vientos
Trichomonas vaginalis is a protozoan flagellate that is a member of a triad group of organisms responsible for the majority of cases of vaginitis / urethritis. The other two organisms included in the group are Candida albicans (and to a lesser degree other Candida spp.) and Gardenerella vaginalis (or otherwise called Bacterial vaginosis (BV) with Gardenerella vaginalis being present along with a host of other bacteria (anaerobes / spirochetes) resulting in a symbiotic pathogenesis.
In women vaginitis is the leading cause of clinic visits. Some 10 million visits per year occur due to vaginitis symptom complaints.
Previously the gold standard was detection by culture. A cumbersome test procedure that required specimens to be brought to the lab within one hour of collection. The sensitivity, while higher than direct techniques such as the microscopic observation of urethral/vaginal wash specimens under microscopic observations, is low especially in low volume infections. Additionally it is important that the organism seen in the microscopic examination be be observed as being motile. The size of Trichomonas vaginalis is typically 10-25 um in length while that of a neutrophil is 12-15 um which can make it difficult to distinguish the two in the microscopic examination. Identification of the organism requires then the observation of motility. The flagella should be seen slashing back and forth.
With the advent of NAAT (nucleic acid amplification tests) and its superior sensitivity of 90% or greater, a sensitivity of 44% for culture was not acceptable. Today there are a myriad of NAAT in the market that test for Trichomonas vaginalis with high sensitivity and specificity. Better yet, there are manufacturers that produce NAAT’s that will detect the main triad of organisms causing vaginitis. In our laboratory we use the Cepheid Xpert Express MVP (Multiplex Vaginal Panel) cartridge which detects not only targets for Candida albicans, Trichomonas vaginalis, and Gardnerella vaginalis, but also cover Candida group/C. glabrata/C. krusei, and other BV indicator organisms. This, we believe, adds an unparalleled opportunity for the detection of the triad of vaginitis causing pathogens. However, the test is only FDA approved for females. A separate test, Xpert TV (Trichomonas Vaginalis) by Cepheid, provides an NAAT that will test for Trichomonas vaginalis in both males and females. This test requires urine specimens for males and both vaginal and urine for females. The test does not however test for the other common causes of vaginitis / urethritis. Both tests take between 40-63 minutes and are conveniently on demand. Most other NAAT are batch mode and not on demand.
While in this particular patient the Trichomonas vaginalis was detected in the urine sediment analysis, this is not the recommended method of detection when suspicious of a Trichomonas vaginalis vaginitis / urethritis. The sensitivity is poor and therefore is not acceptable. This was considered an incidental finding but nevertheless an important reportable result.
PATHOLOGY
Much like the triad responsible for vaginitis and urethritis, Trichomonas vaginalis is considered predominantly sexually transmitted, though transmission can occur through contact with various fomites. The incidence of Trichomonas infections in men is significantly lower than that of women. Infections in both sexes can be asymptomatic, however in women it is significantly more often symptomatic. Because of this propensity for asymptomatic presentations, the organism is easily transmissible to a sexual partner(s) and is therefore an especially problematic sexually transmitted infection (STI) to cure in a sexually active population group.
Symptoms of an infection with Trichomonas vaginalis in men are generally asymptomatic. When symptoms are present in males they may be mild, but of enough intensity to have the infected individual seek help. Symptoms can include dysuria, urethritis, and a generally clear to slightly purulent discharge. In women the intensity of the infection will have them seek help and generally consists of vulvovaginal irritation, a foul odorous vagina, and a copious discharge that is described as yellow-greenish in color. In some women an examination of the cervix will present as having a strawberry-red appearance or what is called colpitis macularis.
Trichomonas vaginalis infections, once considered considered an inconsequential infection, has shown in to be otherwise. Various studies have shown over the years that the organism can have adverse sexual and reproductive health consequences in both males and females. These consequences are a result of repeated or unresolved chronic infections. In males there is an association of chronic infections and prostate cancer, infertility, as well as a higher incidence of HIV. In females there is an association with an increase in HIV as well as infertility. Pregnant females are also at a higher risk of having premature births.
TREATMENT
The first-line effective treatment of Trichomonas vaginalis are 5-nitroimidazole medications. These include metronidazole (MTZ), tinidazole (TDZ), and secnidazole (SEC). It is very important to also treat contacts in order to effectively eradicate the infection in the patient. The failure to treat contacts concomitantly is the main reason for failure to eradicate the infection in patients with recurrence not uncommon. Another reason for failure can be antibiotic resistance. When suspected it is advised to have the organism checked for susceptibility and/or change the antibiotic being used initially. Susceptibility testing is offered by the CDC and other specialty labs.
REFERENCE:
Trichomoniasis. Olivia T Van Gerwen 1, Skye A Opsteen 2, Keonte J Graves 1, Christina A Muzny 1Infect Dis Clin North Am. 2023 Mar 31;37(2):245–265 doi: 10.1016/j.idc.2023.02.001